| Secondary endpoint | Scale | Meaningful risk-factor |
|---|---|---|
| Module 1 (Motivation) | ||
| Corrections Victoria Treatment Readiness Questionnaire (CVTRQ) | Total score | Treatment readiness1 |
| Readiness to Change Questionnaire (RCQ) | Total score | Motivation to change2 |
| Module 2 (Supervision and Social Relationships) | ||
| Social Support Questionnaire (F-Soz-U) | Total score | Negative social influences |
| Optimized Questionnaire for the Measurement of Psychological Reactance (OQMPR) | Total score | Resistance to rules and supervision |
| University of California Los Angeles Loneliness Scale (UCLA) | Total score | Emotionally intimate relationships with adults |
| Module 3 (Emotion Management) | ||
| Barratt Impulsiveness Scale-15 (BIS-15) | Total score | (lifestyle) Impulsiveness |
| Coping Using Sex Inventory (CUSI) | Total score | Sexualized coping |
| Difficulties in Emotion Regulation Scale (DERS) | Subscale Impulsivity | Impulse control difficulties |
| Negative Affect Repair Questionnaire (NARQ) | Subscale Externalized Coping | External Coping |
| Module 4 (Problem Solving) | ||
| Social Problem-Solving Inventory Revised (SPSI-R) | Total score | Poor problem solving skills |
| Module 5 (Offense-Supportive Attitudes) | ||
| Bumby Molest Scale (BMS) | Total score | Offense-supportive attitudes |
| Module 6 (Sexuality Module) | ||
| The Explicit Sexual Interest Questionnaire (ESIQ) | Total score | Sexual interest in children |
| Sexual Outlet Inventory - Revised (SOI-R) | Total score | Sexual interest in children |
| Specific self-efficacy for modifying Sexual Interest in Children (SSIC) | Total score | Self-Efficacy for Modifying Sexual Interest |
| Questionnaire on Emotional Congruence with Children-Revised (EKK-R) | Total score | Emotional congruence with children |
| Hyper-sexualBehavior Inventory-19 (HBI-19) | Total score | Sexual preoccupation |
| 1 Treatment readiness is not defined as a risk-factor in Seto et al. (2023) or Mann et al. (2010). Nevertheless, Treatment dropout is correleated with recidivism. | ||
| 2 Motivation to change is not defined as a risk-factor in Seto et al. (2023) or Mann et al. (2010). Nevertheless, Treatment dropout is correleated with recidivism. | ||
Journal: THE LANCET Digital Health [info; author guidelines]
•
Vers.
0.9.0;
January 30, 2026
Effectiveness of a web-based intervention for individuals who committed sexual offenses against children: a concealed, prospective, parallel group, placebo-controlled, randomized trial in Germany.
Manuscript info
Abstract:
372 words (300 max)
Manuscript:
5457 words (4.500 max)
References:
32 (max 30 references)
Affiliations & Notes
a
Clinic for Psychiatry and Psychotherapy – Forensic Psychiatry, University Medical Center Göttingen, Göttingen, Germany
b
Scientific Core Facility for Medical Biometry and Statistical Bioinformatics, University Medical Center Göttingen, Göttingen, Germany
c
Institute for Sex Research, Sexual Medicine & Forensic Psychiatry, Center for Psycho-social Medicine, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
d
Centre for Criminology, Wiesbaden, Germany
e
Criminal Law, Criminal Procedure, and Criminal Policy, University of Cologne, Cologne, Germany
f
Massregelvollzugszentrum Niedersachsen, Moringen, Germany
g
Clinic for Forensic Psychiatry and Psychotherapy, KRH Psychiatry Wunstorf, Wunstorf, Germany
h
Institute of Social Medicine and Health Systems Research (ISMHSR), Otto-von-Guericke-University Magdeburg, Magdeburg, Germany
Summary
Background
Child Sexual Abuse (CSA) and Child Sexual Exploitation Material (CSEM) offenses cause severe harm. While tertiary prevention programs are well studied in-person, evidence for secondary prevention remains limited, particularly for CSEM-specific programs. Increasing numbers and limited outpatient treatment create post-release care gaps. Web-based interventions (WBIs) may improve access, but empirical evidence for Individuals who have committed CSA or CSEM Offenses (ICCO) is scarce. Only one guided WBI showed small effects on CSEM viewing, but with low conviction rates in the sample. To date, no WBI has been evaluated for ICCO.
Methods
This placebo-controlled RCT was conducted online with 1:1 randomization. Eligible participants were all ICCO under community supervision in Germany. The WBI comprised six guided cognitive-behavioral modules on meaningful risk factors; the placebo delivered psycho-education on healthy-living. Primary outcome was the Child Sexual Abuse Risk Evaluation Self-Report (CARES). Analysis followed intention-to-treat principles using MMRM with treatment group, time, treatment-by-time interaction, baseline CARES, and strata as fixed effects. Secondary outcomes included self-reports on meaningful risk-factors and were analyzed using non-parametric Bonferroni-Holm corrected Brunner-Munzel tests. The trial was prospectively registered (DRKS00021256) and is closed.
Findings
Of 385 screened individuals, 369 were randomized (182 placebo, 187 intervention); 213 included in analysis. The primary outcome showed no significant treatment effects over time (all p≥0·15). Self-reported child sexual interest decreased (ESIQ, padj=0·016) in the intervention arm. Adverse events were rare. The intervention arm required longer to complete some modules (all p≤0·046), but therapeutic alliance (WAI-SR) improved significantly (p≤0·006). No safety concerns were reported.
Interpretations
This first RCT on a WBI for ICCO found no superiority over a online placebo in reducing dynamic risk-factors. The null result aligns with recent meta-analyses showing smaller effects in high-quality studies. High dropout, prolonged module completion, and low baseline risk may have attenuated detectable effects. While the CARES is a promising new measure, its link to official recidivism remains unverified. A small reduction in self-reported sexual interest in children and robust improvements in therapeutic alliance suggest potential benefits. Implementation is not justified without re-working the WBI.
Funding
The work was funded by the German Federal Ministry of Education and Research (BMBF, Funding number: 01KR1807A). The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Research in context
Evidence before this study
Before undertaking this study, no published data on the efficacy of web-based interventions (WBI) in reducing risk-factors of individuals who committed CSA or CSEM offenses was available. The results of the literature search have been published online 2021. A placebo-controlled RCT of a WBI exclusively for CSEM users has been reported for the first time in 2022. The RCT demonstrated a small, but significant reduction of time spended on viewing CSEM based on self-reports (Cohen’s d 0·18). The RCT involved 160 individuals with CSEM use but only 6.9% had prior convictions, limiting generalization to individuals who committed CSA or CSEM offenses. In 2024, an updated review revealed no further empirical evidence. A systematic search was conducted in PubMed, PsycINFO, Scopus, and Web of Science from January 2024 to March 2025 using the terms (“web-based intervention” OR “digital intervention”) AND (“child sexual abuse” OR “child sexual exploitation material” OR “pedophilia”) AND (“recidivism” OR “re offense” OR “risk factor”) AND (“randomized controlled trial”). Results indicate, to the best of our knowledge, that no data on effectiveness of WBIs for individuals who committed CSA or CSEM offenses is published yet.
Added value of this study
The study is the first RCT to evaluate a WBI specifically designed for individuals who have committed CSA or CSEM offenses. It addresses a critical gap in the literature by assessing the effectiveness of a WBI in reducing dynamic risk factors among a population, which has not been previously evaluated. Unlike prior studies focusing on secondary prevention with minimal conviction history, this trial targets ICCO with a structured, modular WBI based on empirical meaningful risk-factors. This RCT provides first preliminary evidence on the impact of a WBI for individuals who have committed CSA or CSEM offenses.
Implications of all the available evidence
The current evidence base indicates that tertiary in-person treatment programs reduce recidivism in individuals who have committed CSA offenses, the empirical evidence for individuals with CSEM offenses is not as well studied. Besides this encouraging results, for individuals who have committed CSA or CSEM offenses access remains limited during community supervision. WBIs offer a promising avenue to bridge the post-release care gap. While preliminary evidence exists for WBIs in secondary prevention, this study adds preliminary support for individuals who have committed CSA or CSEM offenses. Future research must evaluate official re-offense data, and needs to focus on improving engagement and adherence to digital interventions.
Introduction
Child Sexual Abuse (CSA) constitutes one of the most severe adverse experiences in child development.1 Beyond its profound short- and long-term consequences for survivors, CSA represents a substantial challenge for society due to high economical costs2. These figures clearly demonstrate the importance of preventing CSA and CSEM.
In prevention, a distinction is commonly drawn between primary, secondary, and tertiary prevention programs. Primary initiatives are directed at children and their parents, whereas secondary prevention seek to engage adults identified as being at risk for CSA or CSEM, but have not yet been convicted. Tertiary programs have the longest history and are designed for Individuals who already committed CSA or CSEM Offenses (ICCO).2 In recent years, more and more secondary prevention programs for ICCO have been implemented.3 However, a recent meta-analysis identified only five publications exploring the effectiveness of secondary prevention for ICCO, none of them with a methodological high quality.2,3 Thus, currently it is not possible to draw meaningful conclusions on the effectiveness of secondary treatment programs.3 The effectiveness of tertiary programs for ICCO has been studied extensively. In a recent meta-meta analysis, including 21 meta-analyses on tertiary treatment programs, a overall treatment effect with an odds ratio (OR) of 0·67 was reported.4 Several moderators have been identified: community treatment programs provide higher effect-sizes than institutional programs, individualized programs show higher effect-sizes than group programs, high-intensity programs are more effective than low-intensity programs, and the higher the methodological quality, the lower the effect size.4,5 Up to now, most of the meta-analyses report on tertiary programs for individuals who have been convicted for CSA. The figure for CSEM is not as well studied. A recent review demonstrated preliminary support for the effectiveness of secondary prevention programs, but also shed light on the methodological weakness of existing studies on the effectiveness of prevention programs for individuals who have used CSEM: mostly, they suffer from small sample sizes, too short follow-up periods and a lack of officially registered re-offenses as outcome measure.6 Thus, for individuals who have been sentenced for CSEM as well as for secondary prevention programs, the empirical proof of effectiveness is still pending.
Originating from only having few possibilities of community-based treatment offers (e.g. the majority of outpatient therapists working in the primary healthcare system are unwilling to provide treatment) and a rising number of CSEM offenders, there exists a post-release care gap for ICCO .7,8 WBIs are assumed to provide greater accessibility for individuals who face challenges in availing mental health services.9 Thus, it was assumed, that WBIs may bridge the gap in the care of ICCO, but empirical evaluations are scarce.10–12 Schröder et al. identified six WBIs implemented in secondary prevention without published data on their effectiveness.12 Up to now, only one WBI (Prevent It13) reported on it’s effectiveness. The authors evaluated a guided WBI on a sample of 160 individuals who viewed more than five hours weekly CSEM at baseline14 The Randomized Controlled Trial (RCT) showed, that, compared with a psychological placebo, participants of the intervention arm reported a significant, but small decrease in weekly viewing of CSEM (Cohen’s d 0·18). Besides a high dropout rate, this study provides first evidence for the effectiveness of WBIs for secondary prevention of individuals viewing CSEM. Only a minority of the sample reported prior convictions (6.9%).3,11 Data on an updated version are not presented yet.15 Thus, for ICCO, to the best of our knowledge, there exist no proofed WBI yet.
Aim of the study
The study aimed to evaluate the effectiveness of a newly developed WBI @myTabu for ICCO compared to a psychological placebo in a RCT. The primary hypothesis assumes a significant reduction of dynamic risk-factors from baseline to inter-, and post-treatment, compared to a placebo arm. It was further assumed, that each online module within the intervention arm will reduce the dynamic risk-factors targeted in this module in a statistically significant manner.
Method
Study design and participants
The trial was conducted online in Germany and follows a concealed, prospective, parallel group, placebo-control trial with 1:1 randomization. The study design has been prospectively published.16 The trial was prospectively registered on April 24, 2020 in the German Clinical Trial Register (DRKS00021256). The research project was advised by a multidisciplinary team including a representative of participants. All individuals under community supervision (CS; §§56, 57, 68 StGB) from all German federal states (except Hamburg, Bremen, and Saarland), which are sentenced for at least one case of CSA (§§176ff StGB) or CSEM (§184b StGB), were eligible. Exclusion criteria were younger than age of 18 years, a probation period shorter than six months, no access to online intervention, a severe acute psychiatric or cerebro-organic disorder, or a severe cognitive impairment. All participants gave written informed consent. The participants were credited with monetary compensation (€120). However, the participants did not receive any confirmation of having met the treatment requirements set by court . Ethics approval was granted by the medical ethical board of the University Medical Center Göttingen, Göttingen, Germany, on February 21, 2020 (reference number 16/2/20).
Randomisation and masking
The trial comprises two parallel arms (intervention arm and placebo arm). Subjects are randomly allocated to treatment using an allocation ratio of 1:1. The randomization lists are centrally generated using a computerized system (secuTrial®, interActive Systems GmbH, Germany), stratified by the offense type (§176ff StGB vs. §184b StGB), type of CS, external treatment as ordered by court, and static risk to re-offend at baseline (assessed with the modified Static-9917). At screening, each subject receives the next consecutive screening number. At randomization, each subject eligible for study participation receives the next consecutive randomization number according to his stratum from a block of randomization numbers (block size: 4). Due to security reasons, blinding of Supervison Officers (SOs) and Study Therapists (STs) was not possible. Nevertheless, participants, outcome adjudicators, and data analysts were blinded until the end of the data analysis.
Procedures
The concept of the WBI framework, theoretical foundation, and content of the WBI are published online16 and shown in the appendix Section 2 and Figure 1. The content of the trial arms are summarized in Table 1. The WBI builds on already established in-face community-based treatment programs following a cognitive-behavioral approach.18,19 The intervention arm focus solely on psychological meaningful risk-factors.20
| Module | Intervention | Placebo |
|---|---|---|
| Module 1 |
Motivation: – Exercises on identifying personal values and future aspirations in order to enhance treatment readiness and reduce resistance to change. – Psycho-education on improving decision-making by weighting long-term consequences over immediate rewards. – Based on structured goal-setting techniques, participants transform abstract desires into specific, measurable, and achievable objectives, increasing self-efficacy and clarity about their own needs and personal values in order to enhance treatment readiness. |
Physical activity: – Psycho-educational content promotes the benefits of physical activity, identifies personal barriers, and set achievable goals to build motivation for physical activity. – The importance of motor skills, coordination, and balance, enhancing physical confidence and improving participation in daily and therapeutic activities is highlighted. – Through guided exercises, participants are introduced to break sedentary patterns, to increase awareness of health risks and motivated for a sustainable, active living. |
| Module 2 |
Supervision and social relationships: – Development of skills to build trust and collaborative working relationships with supervision officers, reducing resistance against community supervision and improving adherence to supervision mandates. – Identification of avoidance patterns that interfere with engagement in community supervision, using cognitive-behavioral strategies to enhance compliance with structured interventions. – Through guided exercises, participants examine the impact of adult relationships on emotional regulation and behavioral stability, targeting deficits in capacity for adult intimacy. |
Sports: – Psycho-education provides the basics of muscle structure and function, increasing self-awareness of physical capabilities and enhancing motivation to engage in structured physical routines. – In guided exercises, intrinsic and extrinsic motivators are identified as well as barriers like low confidence or time constraints that affect adherence on personal training plans. – By reflecting on personal sport preferences in exercises, participants recognize how peer or cultural influences may shape physical activity choices, reducing susceptibility to negative social pressures. |
| Module 3 |
Emotion management: – Identification of emotions as indicators of unmet personal needs, reducing impulsive reactions by linking affective states to underlying psychological demands. – Through mindfulness exercises and case examples, participants learn the importance of non-reactive awareness of emotions and connected bodily sensations, improving impulse control and reducing maladaptive coping. – Differentiation of emotional experiences and action urges using tools like the tension scale, fostering pause-and-reflect strategies to interrupt impulsive behaviors. – Creation of a personalized skill set, with adaptive, individualized responses to emotional distress, enhancing long-term emotional regulation and self-management. |
Healthy sleep: – Psycho-education promotes that sleep quality directly influences emotional regulation, cognitive function, and physical health, addressing impulsivity and emotional dysregulation that undermine sleep hygiene. – Understanding sleep cycles and physiological restoration helps link poor sleep to heightened stress, supporting those with external or sexualized coping patterns in developing healthier responses. – Practical, non-drug strategies are taught in exercises to manage shift work and jetlag, promoting consistent routines and environmental adjustments that support long-term sleep stability. |
| Module 4 |
Problem solving: – Psycho-education on problem-solving deficits as a core component of self-regulation difficulties, understanding that challenges are manageable through structured, cognitive-behavioral approaches. – Guided exercises following the 7-Step Problem-Solving Plan to systematically identify, define, and address problems, enhancing decision-making and reducing impulsive or avoidant reactions. – Through video examples and case studies, participants practice distinguishing between changeable and unchangeable issues, generating realistic solutions, and evaluating outcomes. |
Dreaming: – Psycho-educational content focus on the neuroscience of dreaming, including REM and non-REM sleep stages. – Through exercises like dream journaling and symbolic interpretation, participants develop reflective practices that enhance awareness of dreams. – The module links stress, sleep disruption, and dream content, illustrating how chronic stress undermines executive function and exacerbates difficulties in structured thinking and solution generation. – Case studies highlight trauma-related dream patterns, showing how unresolved psychological distress and poor sleep hinder insight and cognitive restoration. |
| Module 5 |
Offense-supportive attitudes: – Need-principle: Identification of three offense-supportive cognitions; the participant must choose three out of 16 pre-defined offense-supportive cognitions. – Psycho-education on how offense-supportive cognitions arise from selective attention to partial truths, reinforcing denial and minimizing consequences through psychological defense mechanisms. – Through cognitive restructuring, participants challenge offense-supportive cognitions and promoting critical evaluation of harmful thought patterns in guided exercises. – Case studies and video examples illustrate real-world consequences of offense-supportive cognitions, bridging the gap between perceived justification and actual harm. |
Nutrition: – Adaptive: Psycho-education provides foundational knowledge on nutrition and digestion; the participant must choose three out of six nutrition styles. – Through guided exercises, participants explore ethical, health, and environmental motivations for three out of six different nutrition types (e.g. plant-based diets), fostering empathy and prosocial decision-making. – Practical skills in meal planning and grocery shopping build confidence and sustainability, empowering lasting dietary changes that enhance psychological health and reduce behavioral risk. |
| Module 6 |
Sexuality: – Psycho-education focus on the differentiation between healthy and problematic sexual interests and on how sexual preoccupation can increase reoffending risk. – The module addresses emotional congruence with children as a potential risk-factor, emphasizing the importance of maintaining emotional and physical boundaries between oneself and children to reduce relapse potential (relapse prevention). – Cognitive restructuring techniques are used to challenge distorted beliefs about sexual behavior, fostering insight and promoting adaptive, non-harmful thought patterns. – Through identification of high-risk triggers and personalized coping strategies, the self-regulation, self-efficacy, and control over problematic sexual urges and fantasies will be focused. |
Well-being: – Psychological well-being is distinguished from happiness, focusing on meaning, inner balance, and personal growth, explored through reflections on identity, nature, music, and laughter. – Participants challenge the myth of universal well-being, recognizing its subjective nature and the importance of personal values, identity, and life context in shaping health and satisfaction. – Through exercises, participants explore the gut-brain axis, mindful eating, and hygiene practices, linking nutrition, self-care, and bodily awareness to mental clarity and psychological stability. |
For the recruitment, scientific staff informed SOs about the trial and asked to inform individuals under their supervision. If interested, a meeting with an research assistant (RA) took place at the supervision office. After obtaining the written informed consent, the RA extracted data from official records on site. The WBI was divided into six modules, each module was further divided into four sessions. Participants were advised to walk through one session per week and finish one module in one month. The next session becomes unlocked, when one week has past and all guided exercises have been successfully completed. User tests before running the trial took approximately 60 minutes to complete one session. All endpoints were provided online (see appendix Table 1). Due to ethical reasons, before presenting the questionnaire forms for the primary outcome and the Mood and Risk Questionnaire (MRQ), participants were informed that these answers will be viewable by their SO. To exclude a participant, the SO had to fill in a questionnaire on exclusion reasons (Exclusion Questionnaire, EQ). There was no time constraint defined at which a participant was excluded. Due to data security, the trial staff had no possibility to contact a participant directly. Communication between STs and participants took place online. STs (one male psychotherapist, four female psychologists) were intensively trained by completing a practice online treatment of at least one simulated participant. Regular monthly group supervisions ensured treatment consistency; the answers of STs on guided exercises were manualized (appendix Figure 2). To minimize therapist-related effects, the same STs supported both trial arms.
Outcomes
References, psychometric criteria and descriptions for all outcomes are provided in the appendix Section 3. The Statistical Analysis Plan (SAP), defines officially recorded re-offenses five years after last-patient-out (at September 2030) and the Index of Desistance (IoD) as primary endpoints.16 However, recently, the items of the scales underlying the IoD have been reduced and one scale was removed due to low internal consistency; the IoD was renamed into Child Sexual Abuse Risk Evaluation Self-Report (CARES). The CARES is a composite measure with higher scores indicating greater severity of both acute and stable dynamic risk-factors.21 We report the validated CARES (see appendix section 6.2 for pre-specified IoD).
Secondary endpoints include specific questionnaires operationalizing these risk-factors that are thematically addressed in the individual modules (see Table 2).
Frequencies of re-offenses as reported by SOs were assessed systematicall with the EQ. Frequencies of critical events as reported by STs were assessed continuous (appendix Figure 4), adverse events systematically with the Mood and Risk Questionnaire (MRQ), post-hoc defined as the occurrence of at least one report of the highest possible score on a sub-scale.
The Working Alliance Inventory-Short Revised (WAI-SR) was used to assess therapeutic alliance with STs and SOs. Changes in psychological well-being have been assessed with the WHO-5 Well-Being Index (WHO-5). To assess a possible volunteer-effect, the Questionnaire of Non-Participation (QNP) was developed. The Questionnaire for Acceptance of Technology (ATQ) and the Questionnaire of Subjective Therapy Preconditions (SBV-R) were administered, but not related to the hypotheses and not reported here. Preliminary ATQ data from the intermediate analysis are published.22,23
Statistical analysis
Data analysis was performed using the software R.24 Interim analysis was done by a independent data safety monitoring board (DSMB) on April 20, 2022. Stopping guidelines have been prospectively defined (appendix Section 1).
We found no published WBI for ICCO to guide power calculation, and conservatively assumed small effects . Power analysis revealed a minimum of 214 participants in each arm to be able to detect small effects (d = 0·27) with a power of 80% at a significance level \(\alpha\) = 5%.
Time participants needed to finish the WBI (the time from beginning of module one to the end of the module) and working time ( the time, a participant was working on the content of a module) was analyzed by means of Gaussian linear model for repeated measures (MMRM) with treatment group, time (six time-points), and treatment-by-time interaction.
Statistical analysis for the primary outcome follows the intention-to-treat principle (ITT). The ITT population was defined as all participants who have completed at least one module. The CARES was analyzed by MMRM with treatment group, time (six time-points), treatment-by-time interaction, and the randomization strata as factors, baseline measurements of the outcome, and the CARES as dependent variable. Exploratory, time span from baseline was additionally added to the MMRM as factor. A sensitivity analysis on imputed values complemented the analysis. Imputation was done using multiple reference based imputation followed by ANCOVA models.25 Non-parametric Brunner-Munzel test for paired data (NBMP26) were used to compare the pre- and post-module scores within each trial arm. Differences from baseline were compared between trial arms using the Non-parametric Brunner-Munzel test for unpaired data (NBMU26). If discontinuation from study was due to recidivism, the participant receives the maximal value for the remaining measurements.
To analyze the effects of each individual module, secondary endpoints were analyzed using the NBMP comparing the pre- and post-module scores within each trial arm. Additionally, differences from baseline were compared between the trial arms using NBMU. Secondary endpoints were further analyzed by fitting linear models with trial arm and randomization strata, and pre module scores as factors and post module scores as dependent variable. If the assumptions of a linear model were not fulfilled either an ordinal regression model was fitted analogously instead or the score was dichotomized in order to fit a logistic regression model analogously. Analyses on secondary endpoints were carried out on all participants who provided pre- and post data for the respective module.
Frequencies and percentages of occurrences of re-offenses as reported by the SOs and of self-reported adverse events were compared using Fisher’s exact tests. Ancillaryoutcomes were not pre-specified. The WHO-5 was analyzed by MMRM with treatment group, time (six time-points), treatment-by-time interaction, and the randomization strata as factors, baseline measurements of the outcome and the WHO-5 as dependent variable. The same analysis rationale was applied for the WAI-SR COACH and WAI-SR SUPERVISOR with five time-points.
The error terms of all MMRMs were assumed to follow a multivariate normal distribution with unstructured covariance. Least squares mean changes from baseline are reported for the trial arms with 95% confidence interval (CI) as well as the difference between the least squares treatment group means with 95% CI and p-value testing the null hypothesis of no treatment effect. For all multiple comparisons, p-values were adjusted using the Bonferroni-Holm’s method. All tests were performed two-sided with 5% significance level.
Role of funding source
The work was funded by the BMBF (Funding number: 01KR1807A). The funder had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Results
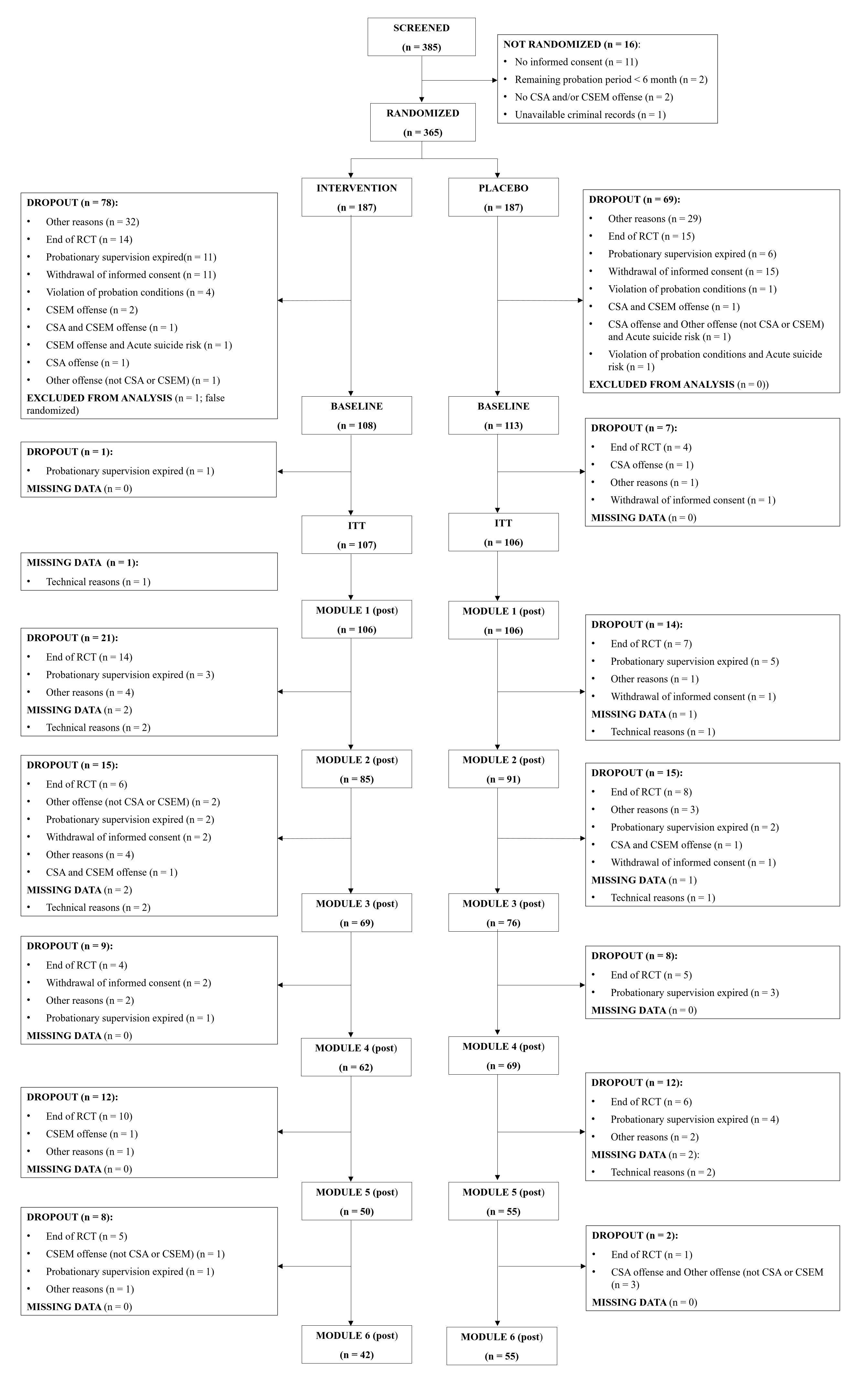
Between March 01, 2020, and September 30, 2024, 385 individuals who committed sexual offenses against children have been screened for eligibility, of whom 16 have not been randomized (see Figure 1). 369 individuals were randomly assigned (182 placebo arm; 187 intervention arm). 213 participants have been included in the ITT sample (107 [57·2%] intervention arm; 106 [58·2%] placebo arm). 99 participants finished the WBI (44 [30·2%] intervention arm; 55 [22·4%] placebo arm). The trial was closed due to end of funding. 70 participants were not able to finish the WBI before closing (39 [59%] intervention arm; 31 [53%] placebo arm).
The trial profile is shown in Table 3. Only two screened participants gave informed consent to fill in the QNP, not allowing any inferences. Participants mean age was 41 years (range 20 to 68), predominantly male (216 [98%]; female: 2 [0·9%]; transsexual: 1 [0·5%]; other: 1 [0·5%]), and with a mean of 13 years of education (range 4 to 21 years). With regard to strata, 89 (40%) participants were mixed offenders (at least one conviction §176ff StG) and 132 (60%) hands-off offenders (only convictions based on $184b StGB). 176 (80%) participants were under CS (§§56, 57 StGB), 45 (20%) under post-release supervision (§§68ff StGB). 70 participants (32%) received an external psychotherapy and/or medical treatment, 151 (68%) not. The court ordered treatment for 124 (56%), for 87 (44%) not. 48 (39%) of all participants, who had an court ordered treatment, received external treatment, 76 (61%) not. 180 participants (81%) had a low to medium static recidivism risk, 41 (19%) a medium to high static risk to re-offend at baseline. The most common psychiatric conditions were other depressive syndromes (20 [9%]), and somatoform syndromes (17 [7·7%]). Psycho-social functioning was generally good (130 [59%] reporting no difficulty at all). Seven (3·2%) participants full-filled the diagnostic criteria for a pedophilic disorder, 213 (97%) not. Data on ethnicity was not assessed.
The mixed model for repeated measures (MMRM) for the primary endpoint showed no evidence of a treatment effect over time (all p≥0·15). Strata as factors had no significant effect (all p≥0·13; see Table 4). Sensitivity analysis (all p≥0·169; appendix Table 8) and a MMRM additionally adjusted for time since the beginning of module one revealed no significance (all p≥0·293; appendix Table 11). Within‑arm pairwise comparisons in the intervention arm showed a significant reduction at module one from median 12 (Q1 8 to Q3 18) to median 12 (Q1 6 to Q3 16, p=0·0050, padj=0·030) and at module 3 from median 11 (Q1 4 to Q3 17) to median 9 (Q1 5 to Q3 16, p<0·010, padj=0·050; appendix Table 9). In the placebo arm, there was a significant reduction at module 1 from median 11 (Q1 7 to Q3 16) to median 9 (Q1 4 to Q3 16, p<0.0001, padj<0.0001), at module two a increase from median 8 (Q1 4 to Q3 16) to median 10 (Q1 4 to Q3 14, p=0.050, padj=0.21), and a decrease at module three from median 10 (Q1 5 to Q3 18) to median 8 (Q1 5 to Q3 14, p=0.041, padj=0.21; appendix Table 10). Change from baseline between trial arms showed no significant effects (all p≥0·052; appendix Table 11). The SAP-conform analysis of the IoD yielded no significant effects (all p≥0·588; appendix section 6.2).
| Characteristic | Overall N = 2211 |
Intervention N = 1081 |
Placebo N = 1131 |
|---|---|---|---|
| Age2 | 42 (20 - 68) | 41 (20 - 66) | 43 (21 - 68) |
| Years of education3 | 13 (4 - 21) | 12 (7 - 21) | 13 (4 - 20) |
| Highest education3 | |||
| No formal education | 17 (7·7%) | 10 (9·3%) | 7 (6·2%) |
| Lower secondary school | 88 (40%) | 42 (39%) | 46 (41%) |
| Intermediate secondary school | 70 (32%) | 36 (33%) | 34 (30%) |
| Upper secondary school | 30 (14%) | 13 (12%) | 17 (15%) |
| University degree | 16 (7·2%) | 7 (6·5%) | 9 (8·0%) |
| Employment status3 | |||
| Unemployed | 61 (28%) | 29 (27%) | 32 (28%) |
| In education/training | 11 (5·0%) | 6 (5·6%) | 5 (4·4%) |
| Unskilled worker | 8 (3·6%) | 5 (4·6%) | 3 (2·7%) |
| Worker | 61 (28%) | 32 (30%) | 29 (26%) |
| Employee | 51 (23%) | 25 (23%) | 26 (23%) |
| Self-employed | 8 (3·6%) | 4 (3·7%) | 4 (3·5%) |
| Retired | 21 (9·5%) | 7 (6·5%) | 14 (12%) |
| Marital status3 | |||
| Single | 144 (65%) | 79 (73%) | 65 (58%) |
| Married | 44 (20%) | 15 (14%) | 29 (26%) |
| Divorced | 29 (13%) | 12 (11%) | 17 (15%) |
| Widowed | 4 (1·8%) | 2 (1·9%) | 2 (1·8%) |
| Gender4 | |||
| Female | 2 (0·9%) | 2 (1·9%) | 0 (0%) |
| Male | 216 (98%) | 105 (97%) | 111 (99%) |
| Trans/Transsexual | 1 (0·5%) | 0 (0%) | 1 (0·9%) |
| Other | 1 (0·5%) | 1 (0·9%) | 0 (0%) |
| Missing | 1 | 0 | 1 |
| Sexual orientation4 | |||
| Exclusively heterosexual | 145 (66%) | 72 (67%) | 73 (65%) |
| Predominantly heterosexual | 24 (11%) | 10 (9·3%) | 14 (13%) |
| Bisexual | 26 (12%) | 12 (11%) | 14 (13%) |
| Predominantly homosexual | 3 (1·4%) | 2 (1·9%) | 1 (0·9%) |
| Exclusively homosexual | 11 (5·0%) | 5 (4·6%) | 6 (5·4%) |
| Asexual | 3 (1·4%) | 3 (2·8%) | 0 (0%) |
| Other | 8 (3·6%) | 4 (3·7%) | 4 (3·6%) |
| Missing | 1 | 0 | 1 |
| Offense type2 | |||
| Hands-on (at least one conviction §176ff StGB) | 89 (40%) | 44 (41%) | 45 (40%) |
| Hands-off (only §184b StGB) | 132 (60%) | 64 (59%) | 68 (60%) |
| Type of supervision5 | |||
| post-release supervision | 45 (20%) | 20 (19%) | 25 (22%) |
| community supervision | 176 (80%) | 88 (81%) | 88 (78%) |
| Static recidivism risk6 | |||
| Low-medium | 180 (81%) | 87 (81%) | 93 (82%) |
| Medium-high risk | 41 (19%) | 21 (19%) | 20 (18%) |
| Term of imprisonment (month)7 | 22 (0 - 156) | 21 (0 - 126) | 23 (0 - 156) |
| Missing | 3 | 1 | 2 |
| Treatment ordered by court7 | |||
| Yes | 124 (56%) | 62 (57%) | 62 (55%) |
| No | 97 (44%) | 46 (43%) | 51 (45%) |
| Additional treatment2 | |||
| Yes | 70 (32%) | 33 (31%) | 37 (33%) |
| No | 151 (68%) | 75 (69%) | 76 (67%) |
| Major depressive syndrome8 | |||
| Yes | 12 (5·4%) | 6 (5·6%) | 6 (5·3%) |
| No | 209 (95%) | 102 (94%) | 107 (95%) |
| Other depressive syndromes8 | |||
| Yes | 20 (9·0%) | 12 (11%) | 8 (7·1%) |
| No | 201 (91%) | 96 (89%) | 105 (93%) |
| Panic syndrome8 | |||
| Yes | 5 (2·3%) | 2 (1·9%) | 3 (2·7%) |
| No | 216 (98%) | 106 (98%) | 110 (97%) |
| Other anxiety syndromes8 | |||
| Yes | 3 (1·4%) | 3 (2·8%) | 0 (0%) |
| No | 218 (99%) | 105 (97%) | 113 (100%) |
| Bulimia nervosa8 | |||
| Yes | 0 (0%) | 0 (0%) | 0 (0%) |
| No | 221 (100%) | 108 (100%) | 113 (100%) |
| Binge eating8 | |||
| Yes | 8 (3·6%) | 3 (2·8%) | 5 (4·4%) |
| No | 213 (96%) | 105 (97%) | 108 (96%) |
| Alcohol syndrome8 | |||
| Yes | 11 (5·0%) | 6 (5·6%) | 5 (4·4%) |
| No | 210 (95%) | 102 (94%) | 108 (96%) |
| Somatoform syndrome8 | |||
| Yes | 17 (7·7%) | 8 (7·4%) | 9 (8·0%) |
| No | 204 (92%) | 100 (93%) | 104 (92%) |
| Psycho-social functioning | |||
| Not difficult at all | 130 (59%) | 60 (56%) | 70 (62%) |
| Somewhat difficult | 76 (34%) | 37 (34%) | 39 (35%) |
| Very difficult | 13 (5·9%) | 10 (9·3%) | 3 (2·7%) |
| Extremely difficult | 2 (0·9%) | 1 (0·9%) | 1 (0·9%) |
| 6D30 Exhibitionistic disorder4 | |||
| Yes | 1 (0·5%) | 1 (0·9%) | 0 (0%) |
| No | 219 (100%) | 107 (99%) | 112 (100%) |
| Missing | 1 | 0 | 1 |
| 6D31 Voyeuristic disorder4 | |||
| Yes | 5 (2·3%) | 4 (3·7%) | 1 (0·9%) |
| No | 215 (98%) | 104 (96%) | 111 (99%) |
| Missing | 1 | 0 | 1 |
| 6D32 Pedophilic disorder4 | |||
| Yes | 7 (3·2%) | 4 (3·7%) | 3 (2·7%) |
| No | 213 (97%) | 104 (96%) | 109 (97%) |
| Missing | 1 | 0 | 1 |
| 6D33 Coercive sexual sadism disorder4 | |||
| Yes | 2 (0·9%) | 2 (1·9%) | 0 (0%) |
| No | 218 (99%) | 106 (98%) | 112 (100%) |
| Missing | 1 | 0 | 1 |
| 6D34 Frotteuristic disorder4 | |||
| Yes | 1 (0·5%) | 1 (0·9%) | 0 (0%) |
| No | 219 (100%) | 107 (99%) | 112 (100%) |
| Missing | 1 | 0 | 1 |
| 6D35 Other paraphilic disorder (non-consenting)4 | |||
| Yes | 1 (0·5%) | 1 (0·9%) | 0 (0%) |
| No | 219 (100%) | 107 (99%) | 112 (100%) |
| Missing | 1 | 0 | 1 |
| Abbreviation: ICD-11 = International Classification of Disease version 11, StGB = German penalty law. | |||
| 1 Mean (Min - Max); n (%) | |||
| 2 data extracted from case files by trained staff (Sample Specifications Questionnaire based on the Court File, SSQ-CF). | |||
| 3 information provided by the participant (Sample Specifications Questionnaire for the Participant, SSQ-P). | |||
| 4 assessed with the ICD-11 screener, a self-report measure which items follow the ICD-11 diagnostic criteria for paraphilic disorders. | |||
| 5 information provided by supervision officer (SSQ-SO); in the German legal system, probation service refers to supervision and support during a suspended sentence or post-release support after prison, while post-release supervision (Führungsaufsicht) is a court-ordered measure of control and assistance after imprisonment in a high security hospital. | |||
| 6 data extracted from case files by trained staff (Sample Specifications Questionnaire based on the Court File, SSQ-CF); since the Static-99 is only defined for hands-on offenders, the reduced Static-99 as mentioned by Seto et al. (2012) was used); all staff member have been trained for the Static-99. | |||
| 7 information provided by supervision officer (Sample Specifications Questionnaire for the SO, SSQ-SO). | |||
| 8 assessed with the PHQ-D. | |||
Analysis of secondary outcomes showed for the intervention arm a significantly decrease in ESIQ from median 87 (Q1 80 to Q3 98) to median 87 (Q1 80 to Q3 90; p=0·0010, padj=0·016), indicating a reduction in sexual interests in children. The SSIC increased from median 28 (Q1 26 to Q3 30) to median 30 (Q1 25 to Q3 30, p=0·049, padj=0·59), the CVTRQ increased from median 85 (Q1 79 to Q3 90) to median 87 (Q1 80 to Q3 92), indicating improved treatment readiness (p=0·0060; padj=0·078), and the DERS increased from median 5 (Q1 5 to Q3 6·5) to median 6 (Q1 5 to Q3 8, p=0·0050, padj=0·070), indicating deterioration of emotion regulation. No other secondary endpoint revealed significance (all p≥0·066; Table 5). In the placebo arm, only the F‑Soz‑U increased from median 3·86 (Q1 3·14 to Q3 4·43) at baseline to median 4 (Q1 3·29 to Q3 4·71) at post‑measurement (p=0·0030, padj=0·045), no other significant differences were observed (all p≥0·12; Table 6). See appendix Table 18 for results of exploratory analyses of change from baseline and appendix Section 7 for results of exploratoryregression models.
| Variable | Beta | 95% CI | p-value |
|---|---|---|---|
| (Intercept) | -0·34 | -1·9 to 1·2 | 0·67 |
| Type of supervision | |||
| community supervision | 0·00 | Ref. | |
| post-release supervision | 0·32 | -1·2 to 1·8 | 0·68 |
| Additional treatment | |||
| No | 0·00 | Ref. | |
| Yes | -0·92 | -2·1 to 0·27 | 0·13 |
| Offense type | |||
| Hands-off (only §184b StGB) | 0·00 | Ref. | |
| Hands-on (at least one conviction §176 ff StGB) | 0·93 | -0·29 to 2·2 | 0·13 |
| Baseline value | 0·84 | 0·77 to 0·91 | <0·0001 |
| Static recidivism risk | 0·38 | -0·13 to 0·88 | 0·14 |
| Timepoint * treatment | |||
| Module 1 (post) * Intervention | 0·39 | -0·83 to 1·6 | 0·53 |
| Module 2 (post) * Intervention | -0·97 | -2·6 to 0·65 | 0·24 |
| Module 3 (post) * Intervention | -0·33 | -1·9 to 1·3 | 0·68 |
| Module 4 (post) * Intervention | -0·25 | -1·8 to 1·3 | 0·75 |
| Module 5 (post) * Intervention | -0·14 | -2·0 to 1·8 | 0·89 |
| Module 6 (post) * Intervention | -0·61 | -2·6 to 1·4 | 0·54 |
| Timepoint | |||
| Module 1 (post) | 0·00 | Ref. | |
| Module 2 (post) | 0·98 | -0·01 to 2·0 | 0·052 |
| Module 3 (post) | -0·46 | -1·4 to 0·50 | 0·34 |
| Module 4 (post) | -0·53 | -1·6 to 0·51 | 0·31 |
| Module 5 (post) | 0·07 | -1·1 to 1·3 | 0·91 |
| Module 6 (post) | 0·16 | -0·97 to 1·3 | 0·78 |
| Abbreviation: CI = Confidence Interval, StGB = German penalty law. | |||
The MMRM for the cumulative time from baseline to finish module showed a significant treatment-by-time interaction across all time-points (all p≤0·035, appendix Table 3). Post-hoc pairwise comparisons showed longer times in the intervention arm for all modules. Unadjusted analyses indicated significant differences at module four (mean 260 days, SD 138, intervention arm; mean 223 days, SD 122, placebo arm; p=0·048) and module five (mean 325 days, SD 161 intervention arm; mean 258 days, SD 113 placebo arm, p=0·028), whereas differences at modules one, two, three, and six did not reach significance (all p≥0·053). After adjustment for multiple comparisons, none remained significant (all q≥0·17; appendix Table 4). The MMRM for the time working on content revealed a significant treatment-by-time interaction at module one (\(\beta\) 360 hours, 95% CI 49 to 671, p=0·024), module four (\(\beta\) 236 hours, 95% CI 19 to 453, p=0·034), and at module five (\(\beta\) 324 hours, 95% CI 6.1 to 641, p=0·046). No significance was observed at module two (\(\beta\) 148 hours, 95% CI -48 to 345, p=0·14), module three (\(\beta\) 188 hours, 95% CI -96 to 473, p=0·19), and module six (\(\beta\) 93 hours, 95% CI -142 to 328, p=0·42; appendix Table 5). Post-hoc pairwise comparisons reveled no differences between trial arms (all p≥0·18; appendix Table 6)
| Characteristic | Pre N = 108 |
Post N = 108 |
p | padj |
|---|---|---|---|---|
| CVTRQ (total score) | 0·0060 | 0·084 | ||
| Mean (SD) | 84 (7) | 86 (8) | ||
| Median (Q1, Q3) | 85 (79, 90) | 87 (80, 92) | ||
| Min, Max | 63, 97 | 64, 100 | ||
| RCQ (total score) | 0·38 | >0·99 | ||
| Mean (SD) | 25·7 (4·0) | 25·2 (4·0) | ||
| Median (Q1, Q3) | 26·0 (23·0, 28·5) | 25·0 (23·5, 28·0) | ||
| Min, Max | 15·0, 33·0 | 12·0, 33·0 | ||
| F-Soz-U (total score) | 0·35 | >0·99 | ||
| Mean (SD) | 3·83 (0·92) | 3·85 (1·04) | ||
| Median (Q1, Q3) | 4·00 (3·14, 4·57) | 4·00 (3·29, 4·86) | ||
| Min, Max | 1·00, 5·00 | 1·00, 5·00 | ||
| Missing | 17 | 17 | ||
| OQMPR (total score) | 0·084 | 0·84 | ||
| Mean (SD) | 29 (9) | 28 (9) | ||
| Median (Q1, Q3) | 29 (23, 35) | 29 (21, 35) | ||
| Min, Max | 12, 52 | 12, 47 | ||
| Missing | 17 | 17 | ||
| UCLA (total score) | 0·066 | 0·79 | ||
| Mean (SD) | 28·5 (3·9) | 28·0 (4·1) | ||
| Median (Q1, Q3) | 28·0 (25·0, 31·0) | 27·0 (24·0, 31·0) | ||
| Min, Max | 22·0, 37·0 | 21·0, 36·0 | ||
| Missing | 17 | 17 | ||
| BIS-15 (total score) | 0·69 | >0·99 | ||
| Mean (SD) | 30 (7) | 30 (8) | ||
| Median (Q1, Q3) | 30 (24, 34) | 29 (24, 35) | ||
| Min, Max | 15, 48 | 15, 48 | ||
| Missing | 36 | 36 | ||
| CUSI (total score) | 0·62 | >0·99 | ||
| Mean (SD) | 29 (9) | 29 (10) | ||
| Median (Q1, Q3) | 28 (25, 32) | 28 (21, 35) | ||
| Min, Max | 16, 66 | 16, 63 | ||
| Missing | 36 | 36 | ||
| DERS (subscale impulsivity) | 0·0050 | 0·075 | ||
| Mean (SD) | 6·24 (2·26) | 6·72 (2·25) | ||
| Median (Q1, Q3) | 5·00 (5·00, 6·50) | 6·00 (5·00, 8·00) | ||
| Min, Max | 5·00, 17·00 | 5·00, 15·00 | ||
| Missing | 36 | 36 | ||
| NARQ (subscale externalizing strategies) | 0·13 | >0·99 | ||
| Mean (SD) | 1·94 (2·74) | 2·11 (2·50) | ||
| Median (Q1, Q3) | 1·00 (0·00, 3·00) | 1·00 (0·00, 3·50) | ||
| Min, Max | 0·00, 14·00 | 0·00, 11·00 | ||
| Missing | 36 | 36 | ||
| SPSI-R (total score) | 0·93 | >0·99 | ||
| Mean (SD) | 13·4 (3·2) | 13·5 (3·3) | ||
| Median (Q1, Q3) | 13·8 (10·4, 16·0) | 13·5 (11·4, 15·6) | ||
| Min, Max | 6·2, 19·8 | 7·4, 19·8 | ||
| Missing | 46 | 46 | ||
| BMS (total score) | 0·35 | >0·99 | ||
| Mean (SD) | 51 (14) | 53 (16) | ||
| Median (Q1, Q3) | 46 (40, 57) | 47 (39, 63) | ||
| Min, Max | 38, 86 | 38, 99 | ||
| Missing | 55 | 55 | ||
| ESIQ (total score) | 0·0010 | 0·016 | ||
| Mean (SD) | 90 (12) | 87 (12) | ||
| Median (Q1, Q3) | 87 (80, 98) | 85 (80, 90) | ||
| Min, Max | 66, 127 | 66, 127 | ||
| Missing | 66 | 66 | ||
| SOI-R (subscale desire for sexual activity with children) | 0·071 | 0·79 | ||
| Mean (SD) | 11 (20) | 9 (21) | ||
| Median (Q1, Q3) | 1 (0, 10) | 1 (0, 5) | ||
| Min, Max | 0, 100 | 0, 100 | ||
| Missing | 66 | 66 | ||
| SSIC (total score) | 0·049 | 0·64 | ||
| Mean (SD) | 26·5 (4·6) | 27·1 (4·3) | ||
| Median (Q1, Q3) | 28·0 (26·0, 30·0) | 30·0 (25·0, 30·0) | ||
| Min, Max | 11·0, 30·0 | 15·0, 30·0 | ||
| Missing | 66 | 66 | ||
| EKK-R (total score) | 0·92 | >0·99 | ||
| Mean (SD) | 30 (8) | 29 (7) | ||
| Median (Q1, Q3) | 28 (24, 35) | 29 (24, 32) | ||
| Min, Max | 20, 54 | 20, 55 | ||
| Missing | 66 | 66 | ||
| HBI-19 (total score) | 0·87 | >0·99 | ||
| Mean (SD) | 30 (12) | 29 (10) | ||
| Median (Q1, Q3) | 25 (20, 40) | 27 (19, 32) | ||
| Min, Max | 19, 57 | 19, 60 | ||
| Missing | 66 | 66 | ||
| Abbreviation: BIS-15 = Barratt Impulsiveness Scale-15, BMS = Bumby Molest Scale, CUSI = Coping Using Sex Inventory, CVTRQ = Corrections Victoria Treatment Readiness Questionnaire, DERS = Difficulties in Emotion Regulation Scale, EKK-R = Questionnaire on Emotional Congruence with Children-Revised, ESIQ = Explicit Sexual Interest Questionnaire, F-Soz-U = Seven-item short version of the Social Support Questionnaire, HBI-19 = Hyper-sexualBehavior Inventory-19, NARQ = Negative Affect Repair Questionnaire, OQMPR = Questionnaire for the Measurement of Psychological Reactance, Q1 = 25th percentile, Q3 = 75th percentile, RCQ = Readiness to Change Questionnaire - German version, SD = Standard deviation, SOI-R = Sexual Outlet Inventory revised, subscale desire for sexual activity with children, SPSI-R = Social Problem-Solving Inventory Revised, SSIC = Specific self-efficacy for modifying Sexual Interest in Children, UCLA = UCLA Loneliness Scale - German short version, padj = Holm-Bonferroni adjusted p-value | ||||
During trial, no critical events were reported by SOs or STs. SOs excluded five (2.3%) participants due to recidivism (two [1.6%] intervention arm; three [2.7%] placebo arm; appendix Table 37). In the MRQ, preparation of contact with children, urges related to CSA, or urges related to CSEM were not reported. Two participants (0·9%) reported planning of a contact with a child (one [0·9%] intervention arm, one [0·9%] placebo arm). Two participants reported suicidal ideations (1.9%), two (1·9%) high sexual tension, and one participant (0·9%) reported losing control of sexual thoughts and activity in the intervention arm, none in the placebo arm. Feeling unable to cope with mental burden was reported by nine (4·1%) participants (7 [6·5%] intervention arm; two [1·8%] placebo arm). A current mental crisis was reported by 15 (6·8%) participants (11 [10%] intervention arm; four [3·5%] placebo arm), and very poor current mood by 12 (5·4%) participants (8 [7·4%] intervention arm; four [3·5%] placebo arm). However, none of these differences was statistically significant (all p≥0·062; appendix Table 35).
For the WHO‑5, the MMRM revealed no evidence for differences between trial arms over time, with no significant treatment-by-time interaction at any time-point (all p≥0·11; appendix Table 38).
The MMRM analyzing the WAI‑SR COACH showed significant treatment-by-time interaction effects at several time-points (\(\beta\) 2·4, 95% CI 0·30 to 4·5, p=0·025 module one; \(\beta\) 3·8, 95% CI 1·2 to 6·5, p = 0·0044 module two; \(\beta\) 3·4 95% CI 0·96 to 5·9, p=0·0067 module three; \(\beta\) 4·3, 95% CI 1·3 to 7·3, p=0·0051 module five). At module four, there was no significant effect (\(\beta\) 2·1, 95% CI -0·63 to 4·9, p=0·13; appendix Table 42). Pairwise comparisons within the intervention arm showed significant increases at module one from median 43 (Q1 34 to Q3 49) to median 47 (Q1 39 to Q3 51, p=0·0020, padj=0·010), and at module five from median 47 (Q1 37 to Q3 57) to median 49 (Q1 41 to Q3 57, p=0·0040, padj=0·016). No other time-point showed significant pre–post changes (all p≥0·21). In the placebo arm, no significant pre–post changes were observed at any time-point (all p≥0·28; appendix Tables 43-44). See appendix Table 45 for exploratorychange from baseline comparisons.
The MMRM analyzing the WAI‑SR SUPERVISOR showed significant treatment-by-time interaction effects at four time-points, except module four (\(\beta\) 2·3 95% CI 0·64 to 4·1, p = 0·0073 module one; \(\beta\) 3·0 95% CI 0·87 to 5·2, p=0·0061 module two; \(\beta\) 3·2 95% CI 1·2 to 5·3, p=0·0022 module three; mean estimate 2·1, 95% CI -0·16 to 4·3, p=0·068 module four; \(\beta\) 3·6 95% CI 1·2 to 6·0, p=0·0038 module five; appendix Table 46). Pairwise comparisons within the intervention arm showed significant increases from median 44 (Q1 36 to 49) to median 47 (Q1 42 to Q3 53, p<0·0001, padj<0·0001) at module one and from 49 (Q1 ) to 50 (SD 8; p=0·046, padj=0·18). No other modules in the intervention arm showed significant pre–post changes (all p≥0·44). In the placebo arm, no significant pre–post changes were observed at any time-point (all p≥0·21). See appendix Table 48 for exploratorychange from baseline comparisons.
| Characteristic | Pre N = 113 |
Post N = 113 |
p | padj |
|---|---|---|---|---|
| CVTRQ (total score) | 0·12 | >0·99 | ||
| Mean (SD) | 85 (7) | 86 (8) | ||
| Median (Q1, Q3) | 86 (81, 91) | 87 (81, 91) | ||
| Min, Max | 67, 100 | 61, 100 | ||
| RCQ (total score) | 0·41 | >0·99 | ||
| Mean (SD) | 25·7 (3·8) | 26·1 (3·5) | ||
| Median (Q1, Q3) | 26·0 (24·0, 28·0) | 26·0 (24·0, 28·0) | ||
| Min, Max | 16·0, 38·0 | 15·0, 32·0 | ||
| F-Soz-U (total score) | 0·0030 | 0·048 | ||
| Mean (SD) | 3·74 (0·84) | 3·88 (0·89) | ||
| Median (Q1, Q3) | 3·86 (3·14, 4·43) | 4·00 (3·29, 4·71) | ||
| Min, Max | 1·71, 5·00 | 1·71, 5·00 | ||
| Missing | 19 | 19 | ||
| OQMPR (total score) | 0·25 | >0·99 | ||
| Mean (SD) | 29 (7) | 28 (8) | ||
| Median (Q1, Q3) | 29 (24, 34) | 28 (22, 33) | ||
| Min, Max | 15, 43 | 12, 47 | ||
| Missing | 19 | 19 | ||
| UCLA (total score) | 0·51 | >0·99 | ||
| Mean (SD) | 28·2 (3·8) | 28·1 (4·7) | ||
| Median (Q1, Q3) | 27·0 (25·0, 30·0) | 27·0 (25·0, 31·0) | ||
| Min, Max | 20·0, 39·0 | 12·0, 42·0 | ||
| Missing | 19 | 19 | ||
| BIS-15 (total score) | 0·96 | >0·99 | ||
| Mean (SD) | 29 (6) | 29 (6) | ||
| Median (Q1, Q3) | 28 (25, 32) | 28 (25, 32) | ||
| Min, Max | 16, 50 | 17, 47 | ||
| Missing | 35 | 35 | ||
| CUSI (total score) | 0·12 | >0·99 | ||
| Mean (SD) | 27 (8) | 28 (8) | ||
| Median (Q1, Q3) | 26 (22, 30) | 28 (23, 32) | ||
| Min, Max | 16, 60 | 16, 59 | ||
| Missing | 35 | 35 | ||
| DERS (subscale impulsivity) | 0·59 | >0·99 | ||
| Mean (SD) | 6·08 (1·75) | 5·92 (1·55) | ||
| Median (Q1, Q3) | 5·00 (5·00, 7·00) | 5·00 (5·00, 6·00) | ||
| Min, Max | 5·00, 13·00 | 5·00, 10·00 | ||
| Missing | 35 | 35 | ||
| NARQ (subscale externalizing strategies) | 0·76 | >0·99 | ||
| Mean (SD) | 1·88 (2·75) | 1·59 (2·12) | ||
| Median (Q1, Q3) | 1·00 (0·00, 3·00) | 1·00 (0·00, 2·00) | ||
| Min, Max | 0·00, 16·00 | 0·00, 11·00 | ||
| Missing | 35 | 35 | ||
| SPSI-R (total score) | 0·82 | >0·99 | ||
| Mean (SD) | 13·54 (2·56) | 13·56 (2·78) | ||
| Median (Q1, Q3) | 13·70 (12·10, 15·20) | 13·80 (11·90, 15·20) | ||
| Min, Max | 6·40, 20·00 | 6·40, 20·00 | ||
| Missing | 41 | 41 | ||
| BMS (total score) | 0·44 | >0·99 | ||
| Mean (SD) | 49 (14) | 48 (14) | ||
| Median (Q1, Q3) | 43 (38, 54) | 42 (39, 53) | ||
| Min, Max | 38, 102 | 38, 102 | ||
| Missing | 54 | 54 | ||
| ESIQ (total score) | 0·62 | >0·99 | ||
| Mean (SD) | 82 (16) | 82 (17) | ||
| Median (Q1, Q3) | 82 (80, 90) | 81 (77, 91) | ||
| Min, Max | 46, 127 | 48, 121 | ||
| Missing | 60 | 60 | ||
| SOI-R (subscale desire for sexual activity with children) | 0·77 | >0·99 | ||
| Mean (SD) | 3 (7) | 4 (9) | ||
| Median (Q1, Q3) | 0 (0, 2) | 0 (0, 1) | ||
| Min, Max | 0, 39 | 0, 47 | ||
| Missing | 60 | 60 | ||
| SSIC (total score) | 0·76 | >0·99 | ||
| Mean (SD) | 27·4 (4·5) | 27·5 (4·4) | ||
| Median (Q1, Q3) | 30·0 (26·0, 30·0) | 30·0 (27·0, 30·0) | ||
| Min, Max | 10·0, 30·0 | 10·0, 30·0 | ||
| Missing | 60 | 60 | ||
| EKK-R (total score) | 0·54 | >0·99 | ||
| Mean (SD) | 30 (8) | 30 (8) | ||
| Median (Q1, Q3) | 27 (25, 35) | 28 (25, 35) | ||
| Min, Max | 20, 54 | 20, 56 | ||
| Missing | 60 | 60 | ||
| HBI-19 (total score) | 0·85 | >0·99 | ||
| Mean (SD) | 26 (8) | 26 (8) | ||
| Median (Q1, Q3) | 23 (20, 28) | 23 (20, 28) | ||
| Min, Max | 19, 55 | 19, 51 | ||
| Missing | 60 | 60 | ||
| Abbreviation: BIS-15 = Barratt Impulsiveness Scale-15, BMS = Bumby Molest Scale, CUSI = Coping Using Sex Inventory, CVTRQ = Corrections Victoria Treatment Readiness Questionnaire, DERS = Difficulties in Emotion Regulation Scale, EKK-R = Questionnaire on Emotional Congruence with Children-Revised, ESIQ = Explicit Sexual Interest Questionnaire, F-Soz-U = Seven-item short version of the Social Support Questionnaire, HBI-19 = Hyper-sexualBehavior Inventory-19, NARQ = Negative Affect Repair Questionnaire, OQMPR = Questionnaire for the Measurement of Psychological Reactance, Q1 = 25th percentile, Q3 = 75th percentile, RCQ = Readiness to Change Questionnaire - German version, SD = Standard deviation, SOI-R = Sexual Outlet Inventory revised, subscale desire for sexual activity with children, SPSI-R = Social Problem-Solving Inventory Revised, SSIC = Specific self-efficacy for modifying Sexual Interest in Children, UCLA = UCLA Loneliness Scale - German short version, padj = Holm-Bonferroni adjusted p-value | ||||
Discussion
In this randomized placebo‑controlled trial of a WBI for ICCO, no superiority of the intervention arm compared to the placebo arm was observed. Among secondary outcomes, only most notably a reduced sexual interest in children was observed. In line with our hypothesis, treatment readiness was enhanced in the intervention arm. Against the hypothesis, difficulties in emotion regulations increased significantly in the intervention arm, whereas the perceived social support increased isolated in the placebo arm. Only in the intervention arm robust significant improvements in the working alliance with STs and SOs were observed. No evidence emerged for an increased risk of recidivism. The frequency of adverse events was generally low without significant differences between trial arms.
Sexual interest in children is considered as the most influential risk-factor for sexual recidivism.20 A central controversy concerns if sexual interests in children is changeable by treatment. While the current clinical paradigm assumes limited changeability, this remains an active scientific debate. Recent meta-analyses reported indications of treatment‑related changes in sexual interest, although none of the included studies employed an adequate control group.27,28 Against this background, the present trial provides evidence for a possible reduction of sexual interest in children by treatment, even compared to a matched control group. However, the magnitude of change was small, warranting cautious interpretation of the clinical significance. The improvements on the working alliance with STs are encouraging, since there is a strong empirical association between working alliance with SOs and recidivism.29
The overall null effect seems to be in line with recent meta-analyses considering in-face treatment programs showing that studies with high methodological quality tend to report smaller or null effects.4,5 Nevertheless, the result contrasts to Lätth et al. who reported a small, but significant effect in favor of the intervention arm on reducing the amount of viewing CSEM.13 Conceptually, the current WBI differs from the WBI in this study, mainly regarding the amount of risk-factors which are targeted, the intensity, and the studied sample, questioning comparability. Previous evidence suggests that higher treatment intensity is generally associated with larger effects4, yet this relationship did not translate into superior outcomes in the present WBI. Meta‑analyses also indicate that treatment targeting high‑risk individuals yield larger effects.4,5 Also dropout rates were high, reports on adverse events were generally low in both RCTs. For the first time, our study provides evidence for ICCO. Several mechanisms may underlie the null findings on the primary outcome. Dropout may have been driven in part by participants’ interest in receiving official documentation for court rather than financial compensation. Baseline static risk-levels were low, suggesting a violation of the need principle of the RNR model by not adapting the content for individual needs.30 Only module five provided individualized treatment content, but failed to show a significant reduction of offense-supportive conditions. Lack of direct contact with participants during the intervention limited participation retention efforts, as reminders could only be communicated via SOs. In consequence, the study was under-powered and small effects remain possibly undetected. Also, psychological burden in the sample was low, which contrasts with previous literature reporting substantial psychological distress.14,31 Self‑reports are controversial discussed, recent evidence suggests that self‑report data can be informative regarding recidivism risk.32 Nevertheless, the CARES is a new instrument, and data linking it to official recidivism outcomes are not yet available.21 Finally, participants in the in both arms required more time to complete modules than advised. Although differences were attenuated after correction for multiple testing, this prolonged duration may have contributed to dropout.
A representative sample was not reached due to data protection regulations. Financial compensation was provided to reduce a potential volunteer bias, but selective referral by probation officers cannot be ruled out. Also, engaging with the WBI necessitated an ability to read German, which is not available to everyone. At the same time, to our knowledge, this is the first RCT evaluating the effectiveness of a WBI for ICCO with a comparable high sample size targeting all meaningful risk-factors with one of the highest sample sizes reported in the literature.
Future research must evaluate official re-offense data, needs to focus on improving engagement and adherence to digital interventions, and should include in-person treatment comparators to clarify the relative effectiveness of the WBI. A stricter RNR‑based individualization, the integration into blended approaches, and a condensation of the content may enhance adherence and effectiveness.
Contributors
PF: writing – original draft, visualization, conceptualization, funding acquisition, project administration, supervision, software, methodology. SSch: writing – review & editing, investigation, methodology, resources, project administration. BS: writing – review & editing, investigation, resources, supervision. ST: writing – review & editing, investigation, conceptualization, resources. AL: formal analysis, visualization, writing – review & editing. FK: formal analysis, visualization, writing – review & editing. LM: writing – review & editing, investigation, methodology, resources. SH: writing – review & editing, conceptualization. CB: writing – review & editing, conceptualization, funding acquisition, resources. KJ: writing – review & editing, project administration. SE: writing – review & editing, conceptualization, funding acquisition. MR: writing – review & editing, conceptualization, funding acquisition. AS: writing – review & editing, conceptualization, funding acquisition. PB: writing – review & editing, conceptualization, funding acquisition. JLM: writing – review & editing, conceptualization, funding acquisition.
Data sharing
The source code, the content of the WBI, and the de-identified data will be made available on reasonable request from the corresponding author (peter.fromberger@med.uni-goettingen.de). Requests, which can be submitted via email to the corresponding author, must include a detailed description of the research question and aims. Data sharing will be authorized following proposal approval and the execution of a signed data access agreement, strictly for scientific use. Code and content sharing follows the same procedure, strictly for non-commercial use.
Declaration of interests
The authors declare no competing interests.
Acknowledgments
The work was funded by the German Federal Ministry of Education and Research (BMBF, Funding number: 01KR1807A). The funder had no role in study design, data collection, data analysis, data interpretation, or writing of the report. A local LLM (Qwen 3) was used for language and grammar correction. The authors are grateful to all participants and SOs for their time, trust and motivation.
References
1
Piolanti A, Schmid IE, Fiderer FJ, Ward CL, Stöckl H, Foran HM. Global Prevalence of Sexual Violence Against Children: A Systematic Review and Meta-Analysis. JAMA Pediatrics 2025; 179: 264–72.
2
Kewley S, Mhlanga-Gunda R, Van Hout M-C. Preventing child sexual abuse before it occurs: Examining the scale and nature of secondary public health prevention approaches. Journal of Sexual Aggression 2023; 29: 1–33.
3
Seto MC, Roche K, Rodrigues NC, Curry S, Letourneau E. Evaluating Child Sexual Abuse Perpetration Prevention Efforts: A Systematic Review. Journal of Child Sexual Abuse 2024; 33: 847–68.
4
Olver ME, Stockdale KC. Sexual Offense Treatment Programming and Recidivism Reduction: A Meta-Meta-Analysis of Program Outcomes and Sources of Effect Size Heterogeneity. Current Sexual Health Reports 2025; 17: 13.
5
Holper L, Mokros A, Habermeyer E. Moderators of Sexual Recidivism as Indicator of Treatment Effectiveness in Persons With Sexual Offense Histories: An Updated Meta-analysis. Sexual Abuse 2024; 36: 255–91.
6
Gouveia C, Silva T, Cunha O, Seto MC, Maimone S, Caridade S. A Systematic Review on the Effectiveness of Interventions for Individuals Who Have Committed Online Sexual Crimes Involving Children. Psychosocial Intervention 2025; 25. DOI:10.5093/pi2025a16.
7
Schmidt A, Niehaus S. Outpatient Therapists’ Perspectives on Working With Persons Who Are Sexually Interested in Minors. Archives of Sexual Behavior 2022; published online Aug. DOI:10.1007/s10508-022-02377-6.
8
Baskurt S. A Meta-analysis of Recidivism Rates Among Individuals Who Commit Child Sexual Exploitation Material (CSEM) Offending. 2024. DOI:10.22215/etd/2024-16307.
9
Crocamo C, Palpella D, Cavaleri D, et al. Digital health interventions for mental health disorders: An umbrella review of meta-analyses of randomised controlled trials. The Lancet Digital Health 2025; 7: 100878.
10
Wild TSN, Fromberger P, Jordan K, Müller I, Müller JL. Web-Based Health Services in Forensic Psychiatry: A Review of the Use of the Internet in the Treatment of Child Sexual Abusers and Child Sexual Exploitation Material Offenders. Frontiers in Psychiatry 2019; 9: 763.
11
Hillert J, Haubrock LS, Dekker A, Briken P. Web-Based Initiatives to Prevent Sexual Offense Perpetration: A Systematic Review. Current Psychiatry Reports 2024; 26: 121–33.
12
Schröder S, Bauer L, Müller JL, Briken P, Fromberger P, Tozdan S. Web-Based Interventions for Individuals who Committed Sexual Offenses Against Children: Development, Evaluation, and Implementation. Criminal Justice and Behavior 2023; 50: 235–51.
13
Lätth J, Landgren V, McMahan A, et al. Effects of internet-delivered cognitive behavioral therapy on use of child sexual abuse material: A randomized placebo-controlled trial on the Darknet. Internet Interventions 2022; 30: 100590.
14
Lätth J, Joleby M, McMahan A, Luke TJ, Rahm C. Child Sexual Abuse Material Users on the Darknet: Psychiatric Morbidities Related to Offence Behavior. Sexual Abuse 2025; : 10790632251347562.
15
HAUBROCk LS, AzEVEDO V, Hillert J, et al. Criminal Police Perceptions of the Internet-Delivered Child Sexual Exploitation and Abuse Prevention Program Prevent It 2.0 in Germany, Portugal, and Sweden.
16
Fromberger P, Schröder S, Bauer L, et al. @myTabu—A Placebo Controlled Randomized Trial of a Guided Web-Based Intervention for Individuals Who Sexually Abused Children and Individuals Who Consumed Child Sexual Exploitation Material: A Clinical Study Protocol. Frontiers in Psychiatry 2021; 11: 575464.
17
Seto MC, Wood JM, Babchishin KM, Flynn S. Online solicitation offenders are different from child pornography offenders and lower risk contact sexual offenders. Law Hum Behav 2012; 36. DOI:10.1037/h0093925.
18
Briken P, Berner W, Flöter A, Jückstock V, von Franqué F. Prävention sexuellen Kindesmissbrauchs im Dunkelfeld – das Hamburger Modell. PSYCH up2date 2017; 11: 243–62.
19
Wild TSN, Müller I, Fromberger P, Jordan K, Klein L, Müller JL. Prevention of Sexual Child Abuse: Preliminary Results From an Outpatient Therapy Program. Frontiers in Psychiatry 2020; 11: 88.
20
Seto MC, Augustyn C, Roche KM, Hilkes G. Empirically-based dynamic risk and protective factors for sexual offending. Clinical Psychology Review 2023; 106: 102355.
21
Sonja Etzler, Katharina Nitsche, Ann-Sophie Tröger, Peter Fromberger, Martin Rettenberger. Development and Initial Validation of the Child Sexual Abuse Risk Evaluation Self-Report (CARES) Scales: Assessment of Acute- and Stable-Dynamic Risk Factors via Self-Report in Individuals Convicted of Sexual Offenses Against Children. submitted; published online submitted.
22
Schröder S, Buntrock C, Neumann L, Müller JL, Fromberger P. Acceptance of a Web-Based Intervention in Individuals Who Committed Sexual Offenses Against Children: Cross-Sectional Study. JMIR Formative Research 2024; 8: e48880.
23
Schröder S, Tozdan S, Briken P, Müller J, Fromberger P. Engagement in a web-based intervention for individuals who committed sexual offenses against children: Observational study. BMC Psychology 2025; 13. DOI:10.1186/s40359-025-02366-z.
24
R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing, 2025.
25
Wolbers M, Noci A, Delmar P, Gower-Page C, Yiu S, Bartlett JW. Standard and reference-based conditional mean imputation. Pharmaceutical Statistics 2022; 21: 1246–57.
26
Brunner E, Munzel U. The Nonparametric Behrens-Fisher Problem: Asymptotic Theory and a Small-Sample Approximation. Biometrical Journal 2000; 42: 17–25.
27
Beggs Christofferson SM, Ealam B. Arousal Management Techniques, Effectiveness and Therapeutic Applications in Sexual Offending Treatment: A Review. Sexual Abuse 2026; : 10790632261417666.
28
Mcphail IV, Olver ME. Interventions for Pedohebephilic Arousal in Men Convicted for Sexual Offenses Against Children: A Meta-Analytic Review. Criminal Justice and Behavior 2020; 47: 1319–39.
29
Sturm A, de Vogel V, Menger A, Huibers MJH. The Price of Mistrust: A Study into the Working Alliance as Predictor for Recidivism. Journal of Police and Criminal Psychology 2022; 37: 576–86.
30
Bonta J, Andrews DA. The psychology of criminal conduct. Routledge, 2023.
31
Chronos A, Jahnke S, Blagden N. The Treatment Needs and Experiences of Pedohebephiles: A Systematic Review. Archives of Sexual Behavior 2024; 53: 3329–46.
32
McMahan A, Luke TJ, Andersson G, Rahm C, Joleby M. Predictive Ability of the Sexual Child Molestation Risk Assessment (SChiMRA+). Sexual Abuse: A Journal of Research and Treatment 2026; : 10790632261415813.